Ocular Toxicities of MEK Inhibitors in Patients With Cancer: A Systematic Review and Meta-analysis
Jing Han, MD, and colleagues examine the prevalence and characteristics of ocular toxicities associated with MEK inhibition.
ABSTRACT
Background: Mitogen-activated protein kinase (MEK) inhibitors, which integrate the important signaling chain of the RAS-RAF-MEK-ERK1/2 pathway, regulate cell functions such as division and proliferation for patients with solid tumors. However, various ocular adverse effects (AEs) affect patients during clinical treatment. This systematic review aimed to assess the occurrence of AEs during treatment with MEK inhibitors plus targeted therapy or chemotherapy.
Methods: A scientific literature search was conducted in PubMed, the Cochrane Library, Embase, and several Chinese databases to identify randomized controlled trials. Overall, ocular AEs were assessed as the primary end point; blurred vision, chorioretinopathy, and retinal detachment were assessed as secondary end points.
Results: Seventeen randomized controlled trials were included. Overall, the use of MEK inhibitors combined with other targeted inhibitors or chemotherapy was significantly associated with a nearly 7.3% increased risk of overall ocular toxicities vs therapy without MEK inhibitors (risk ratio [RR], 2.88; 95% CI, 1.42-5.85, P < .05). An increased risk of blurred vision (RR, 4.10; 95% CI, 2.55- 6.58; P < .05), chorioretinopathy (RR, 8.36; 95% CI, 3.42-20.47; P < .05), and retinal detachment (RR, 8.98; 95% CI, 3.92-20.57; P < .05) was demonstrated.
Conclusions: Treatment with MEK inhibitors combined with targeted drugs or chemotherapy seems to increase overall ocular AEs. A more practical algorithm for the screening of ocular AEs was suggested to be conducted whenever new or worsening ocular toxicities occur.
Oncology (Williston Park). 2023;37(3):130-141.
DOI: 10.46883/2023.25920987
Introduction
MEK proteins are mitogen-activated protein kinase, an important downstream part of the RAS–mitogen-activated protein kinase (MAPK), also known as the RAS-RAF-MEK-ERK1/2 pathway, highly regulating and playing an important role in cell proliferation, differentiation, apoptosis, and stress responses.1 Deregulation of the MAPK pathway occurs in more than 30% of various human cancers.2 Many ongoing clinical trials or preclinical studies of corresponding drugs focus on targeting RAS, RAF, MEK, or ERK. For example, dabrafenib and vemurafenib significantly improved response rates, progression-free survival, and overall survival compared with chemotherapy in metastatic melanoma; however, resistance to treatment developed quickly in most patients. Hitherto, 4 MEK inhibitors have been developed and approved: 3 combined with v-raf murine sarcoma viral oncogene homolog B1 (BRAF) inhibitors to treat several BRAF V600 mutant solid tumors, and 1 for neurofibromatosis type.3-6 Of note, apart from binimetinib, which is used only for melanoma, trametinib has been indicated in combination with dabrafenib for melanoma, non–small cell lung cancer (NSCLC), anaplastic thyroid cancer, and other unresectable or metastatic solid tumors with BRAF V600E mutation in adult patients and pediatric patients 6 years and older.4 Recently, cobimetinib has been newly indicated as a single agent for the treatment of adult patients with histiocytic neoplasms.6
Preclinical studies showed that MEK plays a critical role in maintaining the integrity of the retinal pigment epithelium (RPE) by protecting against various stresses, including oxidative stress, light-induced damage, and inflammation. The RPE is an epithelial barrier formed of RPE cells that maintains the outer blood-retinal barrier and is crucial for maintaining neural retinal function.7 MEK inhibitors lead to acute RPE toxicity, which results in RPE hyperpermeability and breakdown of the retinal-blood barrier. Ocular toxicities are commonly associated with MEK inhibitors, aside from rash, diarrhea, fatigue, and elevated creatinine phosphokinase levels. Thus, this systematic review aimed to provide updated evidence of ocular toxicities related to MEK inhibitors combined with targeted therapy or chemotherapy and briefly discuss their management.
Materials and Methods
Search strategy
We performed a literature search of PubMed, the Cochrane Library, Embase, the Chinese National Knowledge Infrastructure, Wanfang Data, and Chinese Biomedical Literature from inception to November 11, 2020, with the last review performed on January 1, 2022. Keywords included trametinib, binimetinib, selumetinib, cobimetinib, ocular, and eye. A prospective protocol was created in advance and uploaded to the International Prospective Register of Systematic Reviews (PROSPERO) online platform (registration No. CRD42021235589).
Selection criteria and quality assessment
Two reviewers read titles, abstracts, or full texts to identify potential articles that met the inclusion criteria. Studies included in this meta-analysis were required to have (1) a randomized controlled trial (RCT) design, (2) patients with cancer undergoing MEK inhibitor therapy, and (3) eye-related adverse effects (AEs) reported in the outcomes.
Cochrane Collaborations’ tool for assessing the risk of bias was used to assess the quality of included studies by 2 independent researchers. The items included in this tool were random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, and selective reporting.
Data extraction and outcome measures
Two investigators (JH and HZ) independently extracted data from included studies. Disagreements were resolved by consensus or by involving a third review author (JC). Data extracted from studies included study characteristics, patient characteristics, details regarding MEK inhibitor and placebo groups, and outcome measures. The primary end points were clinical events (overall eye-related AEs). The secondary end points incorporated specific ocular AEs (retinal detachment, chorioretinopathy, and blurred vision).
Statistical analysis
This meta-analysis was performed using a statistical software program (Stata version 15.0; StataCorp LP). Outcome data were extracted as risk ratios (RRs) and 95% CIs. Random-effects models were used for all outcomes because of differences in study participants and length of follow-up. The Cochran Q test and the I2 test were performed to assess the heterogeneity of the summary effects. If the P value of the Cochran Q test was less than .01 and I2 was greater than 50%, heterogeneity was considered to exist.


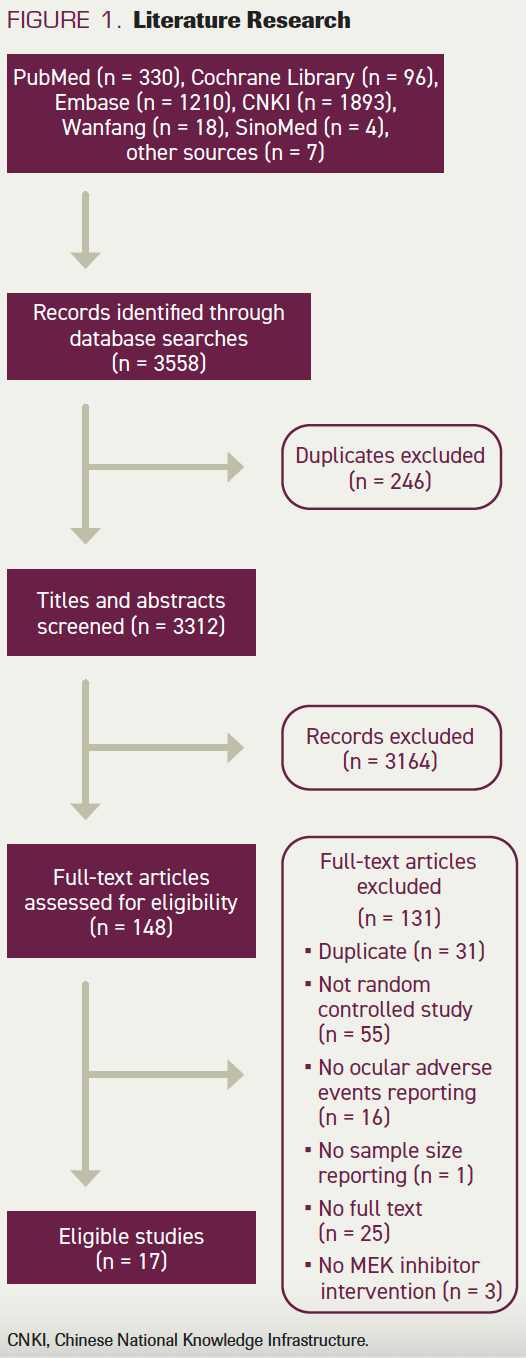
FIGURE 1. Literature Research
Assessment of risk of bias in included studies
Two review authors (JH and HZ) independently assessed risk of bias for each study using the criteria outlined in the Cochrane Handbook for Systematic Reviews of Interventions. We resolved disagreements by discussion or by involving a third review author (JC). We assessed the risk of bias according to the following domains: random sequence generation, allocation concealment, blinding of outcome assessment, incomplete outcome data, selective outcome reporting, and other biases. We graded each potential source of bias as high, low, or unclear risk and provided a quote from the study report together with a justification for our judgment in the risk of bias table. Publication bias was evaluated using a funnel plot of the effect sizes and standard errors of the studies. The Egger regression test was used to examine funnel plot asymmetry. Publication bias was considered to be present if the funnel plot was asymmetrical or the P value from the Egger test was less than .10.
Results
Systematic review and selection
The electronic searches identified 3558 records by searching databases and hand-searching relevant bibliographies. Relevant studies were identified according to the flow diagram in Figure 1. We excluded 246 duplicate records and screened 3312 records, of which 148 were identified as potentially eligible and obtained as full-text manuscripts. After a full-text screening, we considered 17 studies eligible for inclusion in this review.


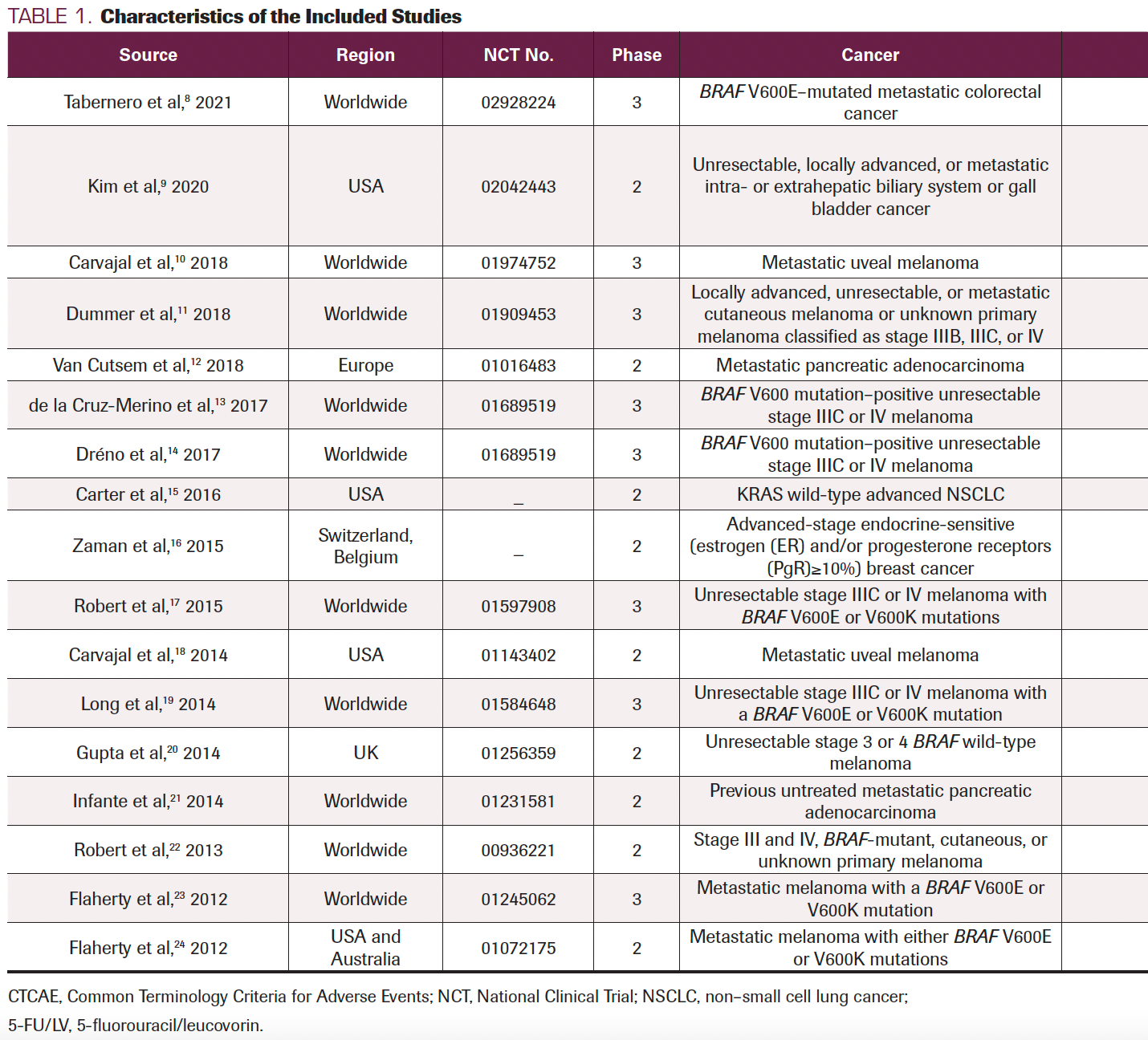


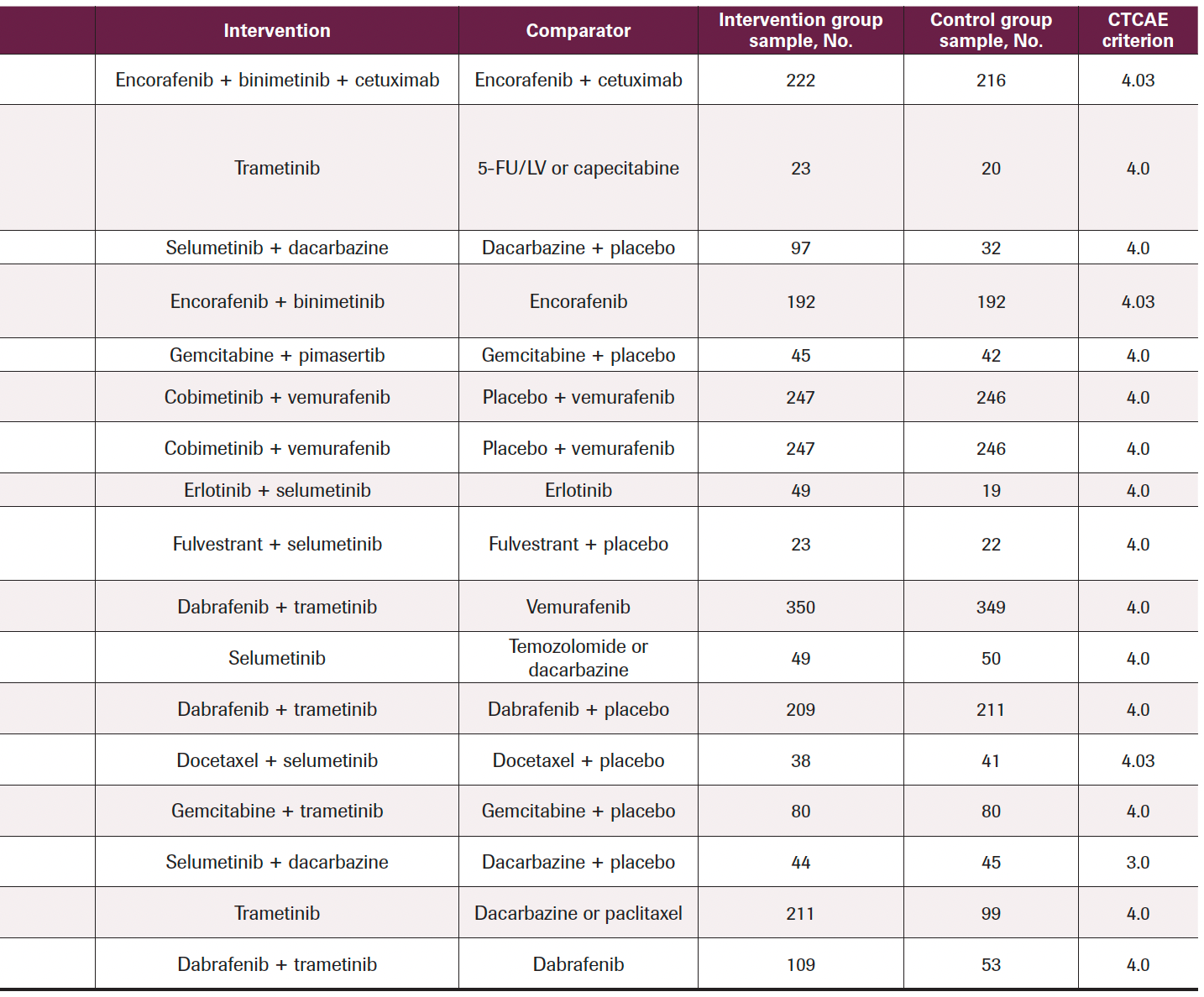
TABLE 1. Characteristics of the Included Studies
Study characteristics
After reading all the text, 17 studies (9 with double-blinded design, 6 with open-label design, 1 with single-blinded design, and 1 with design not mentioned) were included in the final analysis according to the selection criteria, which contained 16 RCTs (Table 1) and the coBRIM clinical trial, which reported secondary end points in 2 studies. Among these studies, 8 were phase 3 and 9 were phase 2, and all included treatment with MEK inhibitors: 3 with a single MEK inhibitor, 9 with a combination of MEK and other targeted inhibitors (such as BRAF inhibitors or epidermal growth factor receptor [EGFR], tyrosine kinase inhibitors, and estrogen antagonists), and 5 with a combination of MEK inhibitors and chemotherapy (such as dacarbazine, gemcitabine, or docetaxel). The MEK inhibitors covered in this study included trametinib, selumetinib, cobimetinib, binimetinib, and pimasertib. In all trials, the pathologic conditions included were colorectal cancer, bladder cancer, melanoma, pancreatic adenocarcinoma, NSCLC, or breast cancer. The criteria used for ocular AE classification was the National Cancer Institute Common Toxicity Criteria for Adverse Events version 3 or 4.
Overall ocular AEs
We performed data analyses for the following comparisons and subgroup analyses. Where applicable, we performed prespecified sensitivity analyses as noted in the Sensitivity Analysis and Risk of Bias section. The use of MEK inhibitors with or without other targeted inhibitors or chemotherapy (vs targeted therapy or chemotherapy without MEK inhibitors) was significantly associated with a nearly 7.3% increased risk of the overall ocular toxicities in a random-effects model meta-analysis of 16 RCTs (RR, 2.88; 95% CI, 1.42-5.85; P < .05) (Figure 2). The risks of all grades of ocular toxicities were 12.4% and 5.1% in the experimental and control arms, respectively.
Subgroup analyses showed that MEK inhibitor monotherapy or therapy with MEK inhibitors plus chemotherapy (vs chemotherapy with or without placebo) was significantly associated with an 8.7% increased risk of ocular AEs in 8 RCTs (RR, 3.82; 95% CI, 1.47-9.91; P < .05) (Figure 2). The risks of all grades of ocular toxicities in this chemotherapy subgroup were 13.3% and 4.6% in the experimental and control arms, respectively.
The results trend for all grades was similar in the targeted therapy subgroup, with 12.0% and 5.3% in the experimental and control arms, respectively. The experimental arms of MEK inhibitors combined with BRAF inhibitors, EGFR inhibitors, or estrogen antagonists (vs BRAF inhibitors, EGFR inhibitors, or estrogen antagonist monotherapy with or without placebo) were associated with a 6.7% increased risk in 8 RCTs (RR, 2.24; 95% CI, 0.79-6.41; P > .05) (Figure 2).
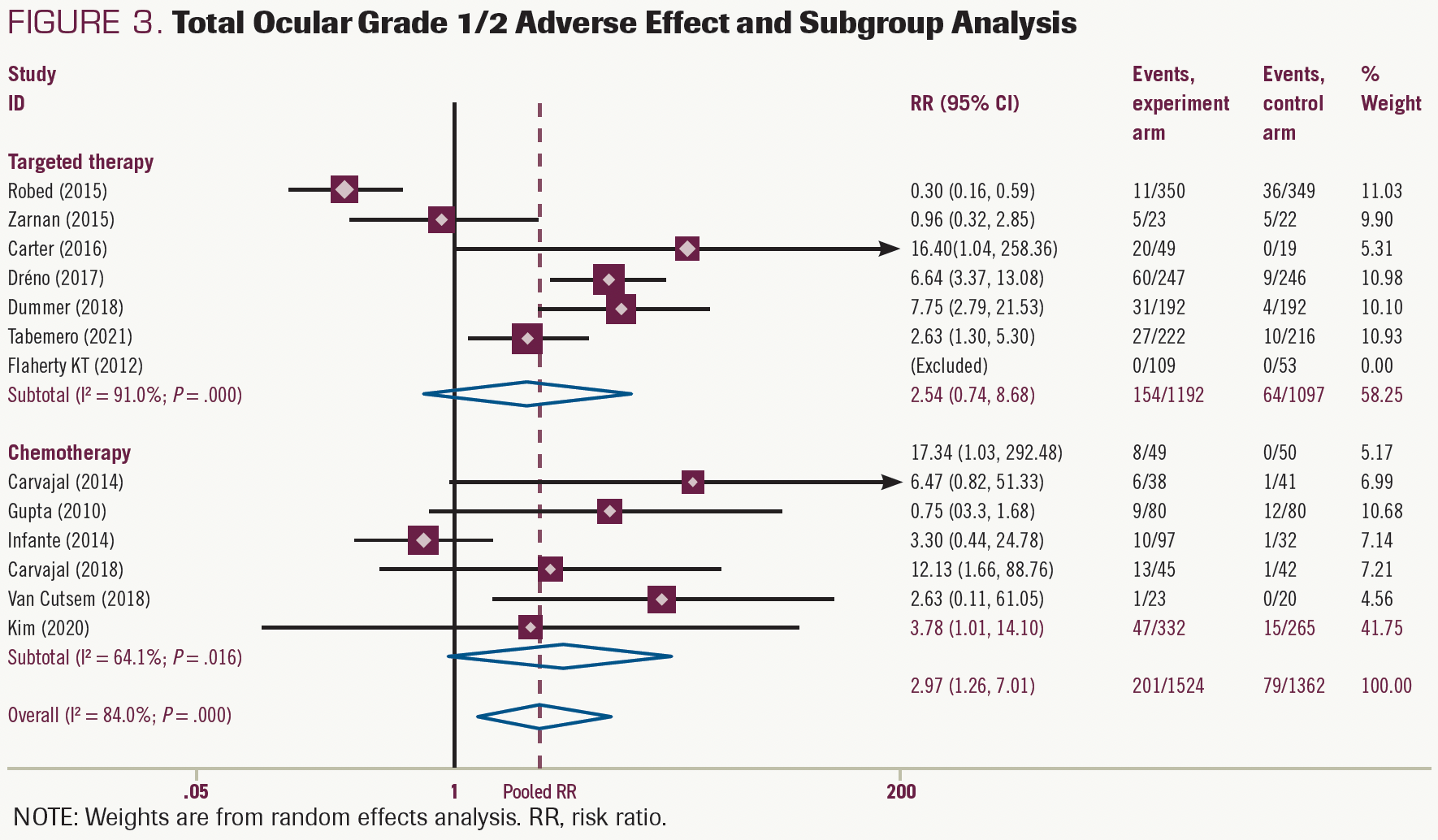
In a random-effects model meta-analysis, MEK inhibitors with or without other targeted inhibitors or chemotherapy (vs targeted therapy or chemotherapy without MEK inhibitors) was significantly associated with a nearly 7.4% increased risk of grade 1/2 ocular toxicities (RR, 2.97; 95% CI, 1.26-7.01; P < .05) (Figure 3). As for chemotherapy subgroups, the pooled results showed that MEK inhibitor monotherapy or MEK inhibitors plus chemotherapy (vs chemotherapy with or without placebo) increased the risk of the grade 1/2 ocular toxicities by approximately 8.5% (RR, 3.78; 95% CI, 1.01-14.10; P < .05) (Figure 3). In the targeted therapy group, therapy with MEK inhibitors tended to increase the occurrence of grade 1/2 ocular AEs, but this increase was not significant (RR, 2.54; 95% CI, 0.74-8.68; P > .05) (Figure 3).
The results for grade 3/4 ocular toxicities were similar when pooling in the targeted therapy subgroup (RR, 7.23; 95% CI, 1.04-50.28; P < .05) (Supplement S1). However, the risk-of-chemotherapy subgroup was presented in 1 article and thus could not be pooled effectively.


FIGURE 2. Total Ocular Adverse Effect and Subgroup Analysis
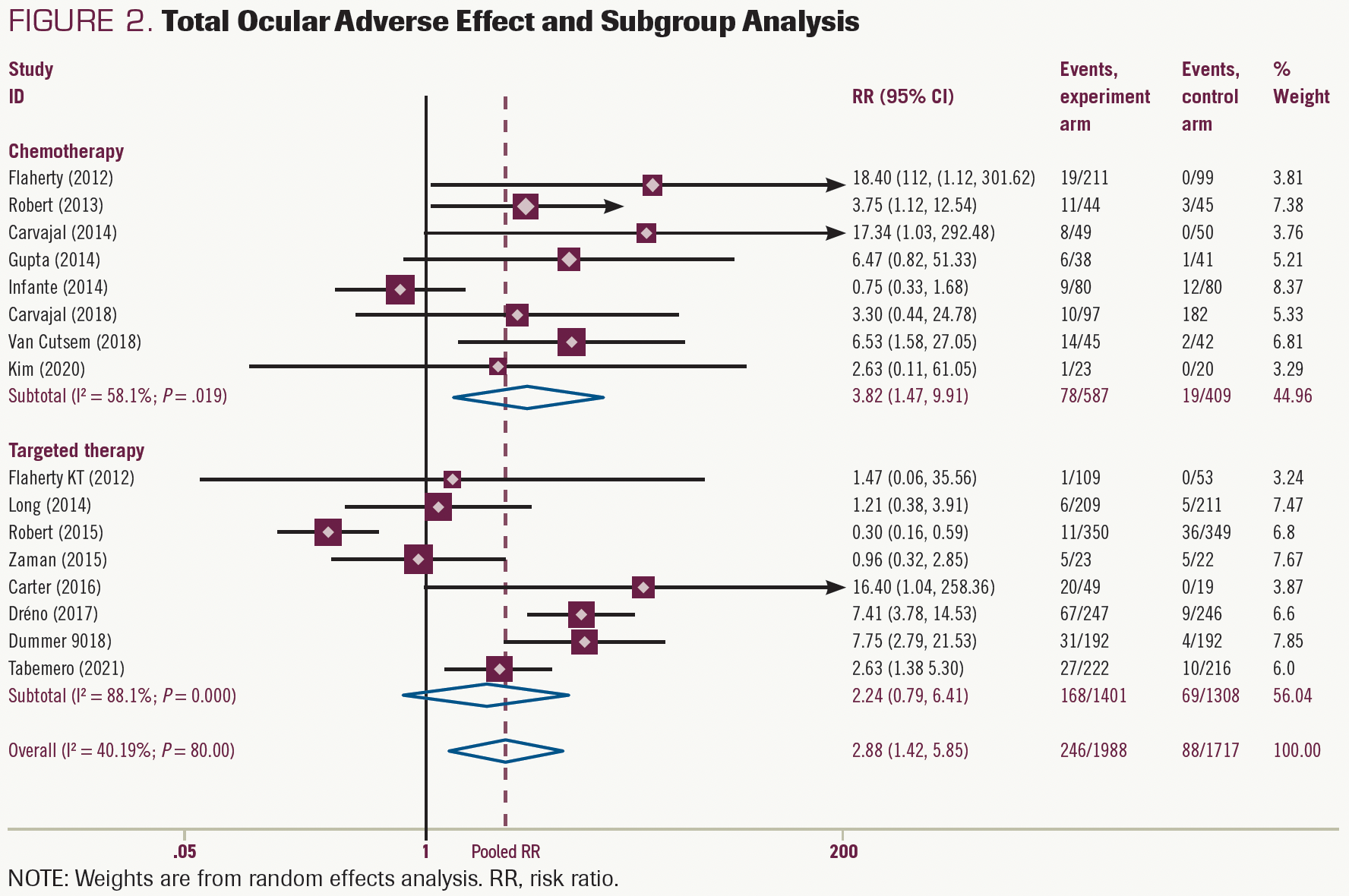


FIGURE 3. Total Ocular Grade 1/2 Adverse Effect and Subgroup Analysis
Secondary end points
Data on blurred vision were extracted from 8 studies. The experimental group of MEK inhibitors was harmful in these studies (RR, 4.10; 95% CI, 2.55-6.58; P < .05) and the same in the chemotherapy group (RR, 4.98; 95% CI, 1.36- 18.17; P < .05) and the targeted therapy group (RR, 3.95; 95% CI, 2.38-6.55; P < .05) (Figure 4). The risk of grade 1/2 AEs was 8.9% higher in the MEK inhibitors experimental group and was 9.6% and 7.3% higher (Supplement S2) in targeted therapy and chemotherapy groups, respectively. No risk of grade 3/4 blurred vision was reported in the included studies.
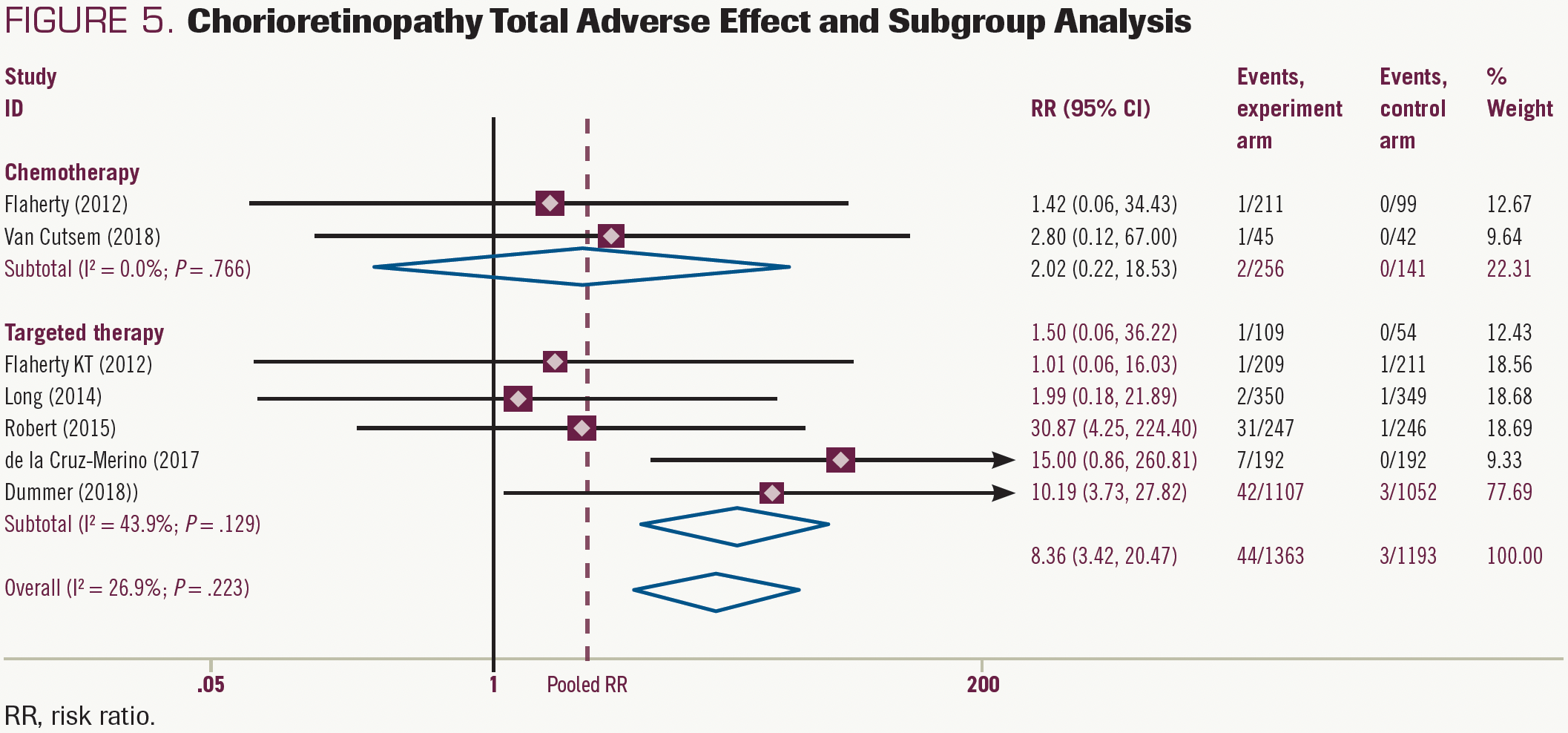
Data on chorioretinopathy was available in 7 studies. MEK inhibitors combined with BRAF inhibitors significantly increased the risk by 3.5% (95% CI, 3.73%-27.82%; P < .05) vs BRAFinhibitor monotherapy (Figure 5). The results for grade 1/2 chorioretinopathy were similar, and MEK plus BRAF inhibitors tended to increase risk (RR, 3.14; 95% CI, 0.83%-13.92%; P >.05), but not significantly (Supplement S3). The risk of grade 3/4 chorioretinopathy was present in 2 articles in the targeted group, an increasing risk tendency but not significant (Supplement S4). In the chemotherapy group, MEK inhibitors with or without chemotherapy (vs chemotherapy alone) did not significantly increase the risk of chorioretinopathy.
Data for retinal detachment were extracted from 3 studies: 2 compared MEK inhibitors plus BRAF inhibitors vs BRAF inhibitors alone, and 1 compared pimasertib plus gemcitabine vs gemcitabine plus placebo. The pooled meta-analysis of these 3 studies showed that the MEK inhibitors group increased the retinal detachment risk by 10.1% (RR, 8.98; 95% CI, 3.92-20.57; P <.05) (Supplement S5) compared with the no MEK inhibitors group.


FIGURE 4. Blurred Vision Total Adverse Effect and Subgroup Analysis
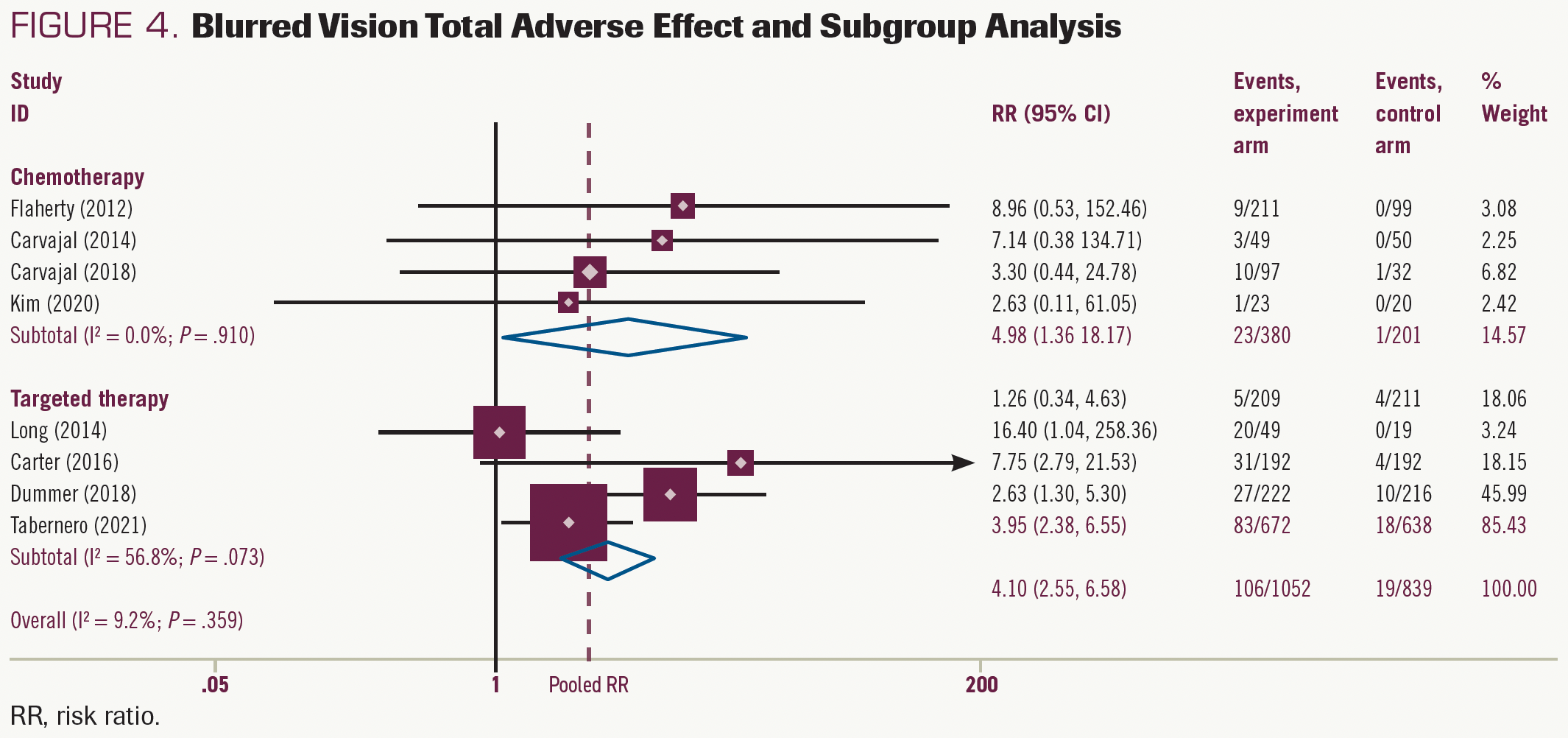


FIGURE 5. Chorioretinopathy Total Adverse Effect and Subgroup Analysis
Sensitivity analysis and risk of bias
To further explore the potential heterogeneity from any single study, sensitivity analysis was performed and showed that the present results were significantly affected by removing 1 study, and the pooled analysis showed increasing ocular toxicities risk in the MEK inhibitors group (Supplement S6). We summarize the risk of bias assessments for the primary outcome of this review in Supplements S7 and S8. We ran a comprehensive search and considered the risk of having missed published reports to be low. The funnel plot of data from the 16 studies included in the meta-analysis was symmetrical (Supplement S9). The P value for the Egger test was .199; there was no publication bias in the meta-analysis (Supplement S10).
Discussion
Clinical manifestations of the MEK-associated ocular adverse effect
During the past decade, newer targeted agents have been developed to exploit tumor-specific genetic alterations in signal transduction pathways, which have taken anticancer therapy into a new era. MEK inhibitors, a crucial part to break the MAPK pathway and a great partner for BRAF inhibitors, especially trametinib, have been developed and approved for use in combination with dabrafenib for early melanoma, specifically for unresectable or metastatic solid tumors with BRAF V600E mutations.25 As the indications expand, the clinical safety of MEK inhibitors should be carefully examined.
Ever since the first MEK inhibitor, CI-1040, was clinically evaluated, ocular toxicities have been regularly reported for this class of drugs.26 Common ocular toxicities included blurred vision and visual disturbances, and these tended to arise quickly after dosing in the first studies with the MEK inhibitors CI-1040, PD0325901, and selumetinib.27,28 Thus, researchers of the phase 1 trials of trametinib suspected these toxicities to be related to the peak concentration. However, because these toxicities are very similar to those reported in newly developing MEK inhibitors, there seems to be a class effect.
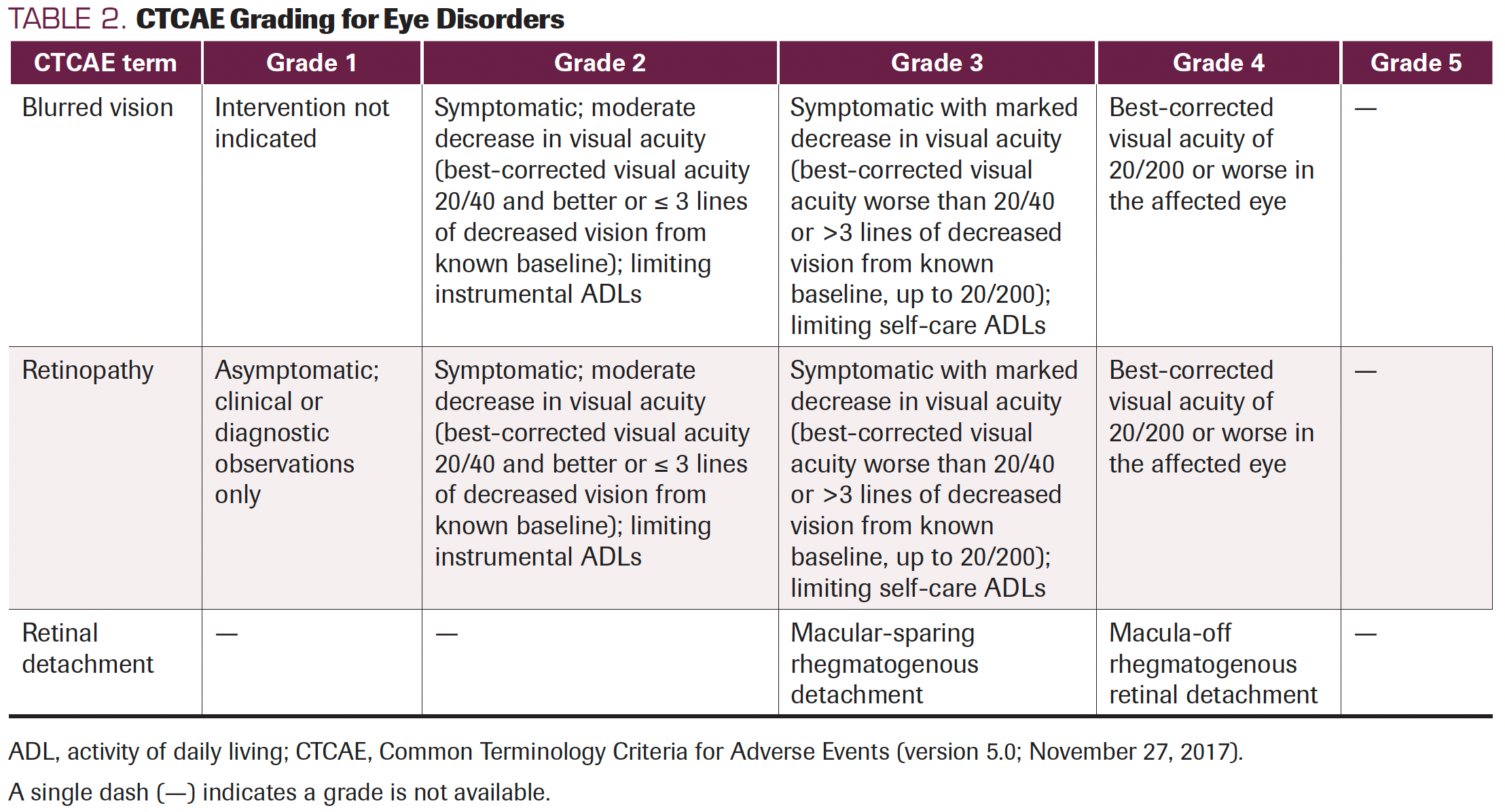
In general, most patients with ocular toxicities identified various clinical manifestations, including reduced visual acuity, blurred vision, dyschromatopsia, chorioretinopathy, retinal detachment, and photophobia.17,29 Herein, blurred vision, chorioretinopathy, and retinal detachment were pooled according to the included studies as secondary outcomes, for they were commonly described as such in the clinical trials. In fact, other types of ocular toxicities, such as cataracts, photosensitivity reactions, macular edemas, and macular fibroses, were also mentioned in 1 clinical trial, but they could not be pooled effectively. In contrast, the secondary end points we chose in this systematic review are consistent with the United States Common Terminology Criteria for Adverse Events evaluation standard (Table 2). Blurred vision represents a disorder characterized by visual perception of unclear or fuzzy images. Chorioretinopathy describes a disorder involving the choroid and retina. Retinal detachment was characterized by the separation of the inner retina layers from the underlying pigment epithelium. Of note, although these 3 toxicities have been classified as grades 1 to 5, most patients experienced grade 1/2 toxicities more often, according to the present results. What’s more, MEK inhibitor–related retinopathy usually begins acutely within 1 week of taking the first dose. Clinical examination in patients with mild disease usually shows multifocal and bilateral small subretinal detachments, possibly with subretinal fluid accumulation. Moderate cases may have only multiple subretinal detachments. More severe cases may develop intraretinal fluid or cysts, as well as disorders of the outer retina. Clinical presentation is usually bilateral, although there are exceptions, and usually symmetrical. Symptoms vary widely; many patients are asymptomatic.


TABLE 2. CTCAE Grading for Eye Disorders
Retinal vein occlusion (RVO) is an uncommon but potentially serious AE reported in initial clinical trials of several MEK inhibitors, including cobimetinib and trametinib. Across all clinical trials, trametinib resulted in an RVO rate of 0.2%.30,31 Predisposing factors included glaucoma, uncontrolled high blood pressure, and diabetes. In at least 1 patient, switching from continuous to intermittent dosing reduced the incidence of RVO.32 At least 1 study has shown that MEK inhibitor–related RVO is associated with hyperhomocysteinemia, an inherited metabolic disease that predisposes to venous thromboembolism. These sparse data suggest that screening for hyperhomocysteinemia before initiation of MEK inhibitor therapy may be beneficial, but more data are needed.33
Differentiating metastasis from drug toxicity
MEK inhibitors as a class of anticancer agents are commonly used in melanoma, NSCLC, and other solid tumor treatments. However, clinicians should distinguish visual disturbances caused by other medical etiologies (such as diabetic complications, hypertension complications, or concomitant medication) from ocular toxicities caused by MEK inhibitors. If the patient has a history of diabetes, hypertension, other diseases, or a special medication history, an ophthalmologic evaluation should be performed before antitumor treatment. The exact etiology can be quickly distinguished when eye symptoms worsen. Of note, apart from these etiologies, tumor eye metastasis may be uncommon but can still happen in clinical practice and should be noted in patients with cancer. Oncologists and ophthalmologists should learn about the common intraocular metastatic lesions, often involving the uvea, which consists of the iris and ciliary body anteriorly and the choroid posteriorly. Choroidal metastases typically present as raised amelanotic choroidopathy with patchy pigmentation of the RPE. They are often accompanied by an upper serous retinal detachment disproportionate to the lesion itself. Symptoms depend on the location of the metastases: peripheral metastases containing a small amount of serous fluid may be asymptomatic, whereas macular involvement or subretinal fluid can cause flash hallucinations (subjective perception of flashes, sparks, or color), visual distortion, floaters, blurred vision, difficulty focusing, and dyschromia (an abnormal ability to perceive colors). Although some of these symptoms may mimic drug toxicity, mydriatic fundus examination (often combined with ocular ultrasonography and optical coherence tomography) can often differentiate choroidal metastases from drug-induced retinopathy.34,35 Orbital or optic nerve metastases can cause optic disc edema, which can be secondary to papilledema due to brain metastases. In such cases, cross-sectional imaging of the head can assist in the diagnosis.36 Retinal metastases can cause retinal inflammation and intraretinal hemorrhage, and vitreous metastases cause the accumulation of white blood cells in the vitreous, which may manifest as vitritis (inflammation of the vitreous body). Mydriatic fundus examination and vitreous biopsy can help differentiate true vitritis from vitreous metastases.37
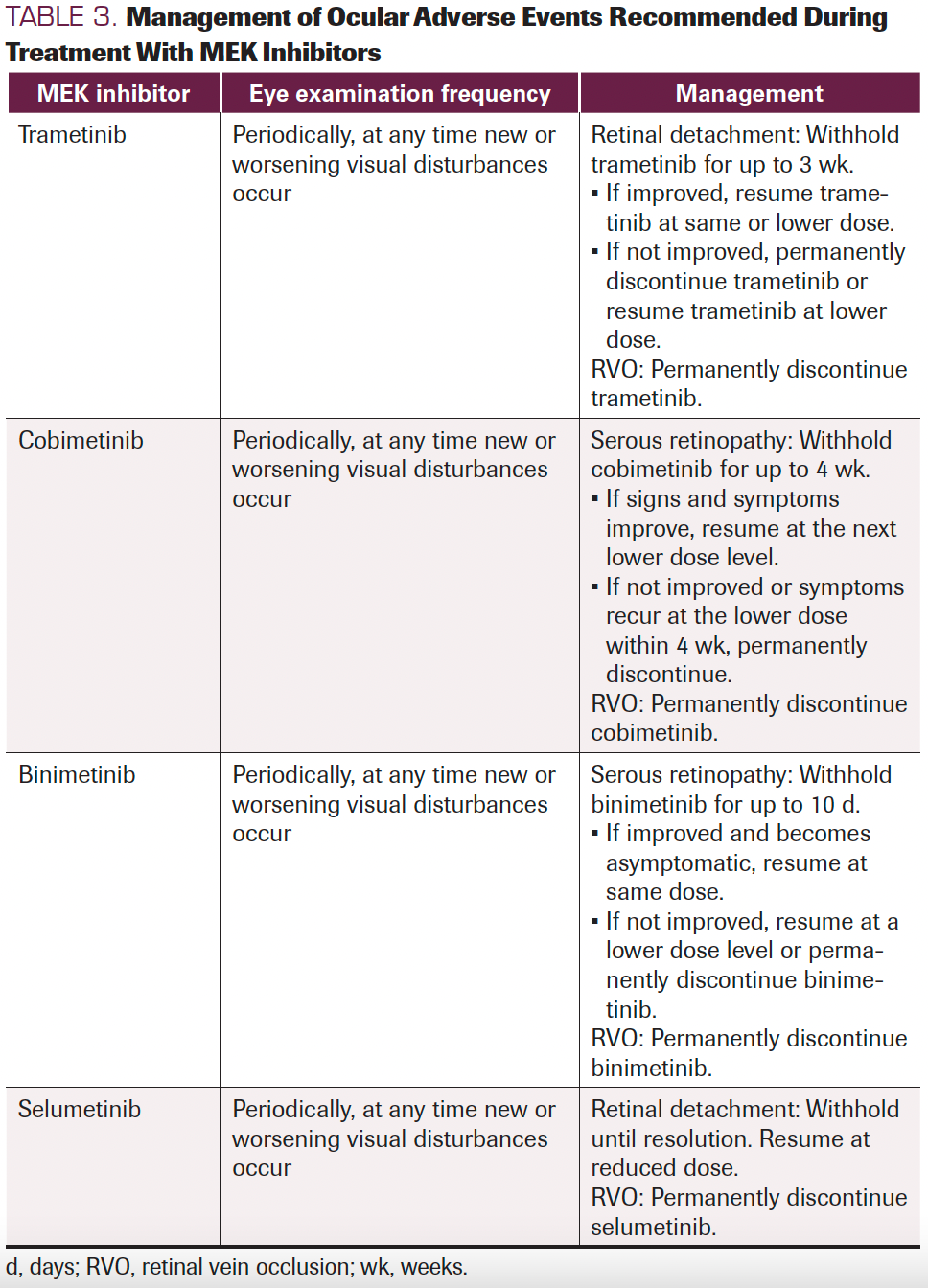
Management of ocular AEs associated with MEK inhibitors
The US package inserts for trametinib and cobimetinib recommend that patients receive regular eye examinations during treatment and whenever new or worsening visual disturbances occur. Because most ocular toxicities are mild or moderate (and almost always reversible), patients and oncologists should pay attention to these AEs, but more comprehensive ophthalmology evaluations should be received at the onset of clinical symptoms. If retinal detachment has been diagnosed, trametinib should be withheld; it should be restarted at the same or a lower dose only if the retinal detachment resolves within 3 weeks. Clinicians should discontinue the drug, or restart at a lower dose, if there is no improvement after 3 weeks, if the disease recurs, or if RVO occurs. For serous retinopathy caused by cobimetinib, treatment should be interrupted until visual symptoms improve. Treatment can be resumed at a lower dose only if symptoms improve within 4 weeks. Clinicians should permanently discontinue treatment if symptoms recur or RVO occurs. In a similar vein, if serous retinopathy is caused by binimetinib, treatment should be withheld and then resumed at a lower dose if symptoms improve within 10 days. Otherwise, permanently discontinue if no improvement or RVO occurs. Moreover, selumetinib was the same (Table 3). Currently, there are no validated treatment options available for retinal detachment and RVO. The fluid accumulation is usually reabsorbed in retinal detachment, with symptoms resolving and no need for treatment. RVO is a more serious AE requiring therapeutic intervention. Drug discontinuation should inform consent from patients first, for they have the right to decide. They may maintain eyesight or suffer blindness under the following MEK inhibitor treatment, drug discontinuation should be carefully evaluated for metastatic patients. A range of treatments, including vascular endothelial growth factor receptor inhibitors, anticoagulants, corticosteroids, and thrombolytic agents, have attempted to solve this problem but have no validated evidence to date.38,39 The lack of available treatment options requires oncologists, ophthalmologists, and patients to mind this problem, and favors ophthalmologic examinations before and after the start of MEK inhibitor treatment to achieve quick diagnoses and close monitoring.


TABLE 3. Management of Ocular Adverse Events Recommended During
Treatment With MEK Inhibitors
Conclusion
MEK inhibitors are novel targeted anticancer agents of the MAPK pathway and have been approved to treat melanoma, NSCLC, and various BRAF V600–mutant solid tumors. However, they seem to cause common and unique ocular toxicities. Treatment with MEK inhibitors combined with targeted drugs or chemotherapy (vs targeted therapy or chemotherapy without MEK inhibitors) seems to increase overall ocular AEs, especially blurred vision, chorioretinopathy, and retinal detachment. To overcome this limitation, oncologists and ophthalmologists need to enhance communication to safeguard patient health during MEK inhibitor therapy.
FUNDING: This work was supported by a grant from the Leading Talent Cultivation Project of Henan Health Science and Technology Innovation Talents (No. YXKC2020009), Henan International Joint Laboratory of Drug Resistance and Reversal of Targeted Therapy for Lung Cancer (No. [2021]10), Henan Medical Key Laboratory of Refractory Lung Cancer (No. [2020]27), and Henan Refractory Lung Cancer Drug Treatment Engineering Technology Research Center (No. [2020]4). The funders had no role in the study design, data collection/ analysis, decision to publish, or preparation of the manuscript.
AFFILIATIONS:
Jing Han, MD1; Juejing Chen, MD2; Hanqiong Zhou, MD1; Lidan Hao1; Qiming Wang, MD, PhD1
1Department of Internal Medicine, The Affiliated Cancer Hospital of Zhengzhou University and Henan Cancer Hospital, Zhengzhou, China
2State Key Laboratory of Ophthalmology, Zhongshan Ophthalmic Center, Sun Yat-sen University, Guangzhou, China
CORRESPONDING AUTHOR:
Qiming Wang, MD, PhD
Department of Internal Medicine
The Affiliated Cancer Hospital of Zhengzhou University
Henan Cancer Hospital
Zhengzhou, China
Email: qimingwang1006@126.com
REFERENCES
- Han J, Liu Y, Yang S, Wu X, Li H, Wang Q. MEK inhibitors for the treatment of non-small cell lung cancer. J Hematol Oncol. 2021 Jan 5;14(1):1. doi: 10.1186/s13045-020-01025-7
- Braicu C, Buse M, Busuioc C, Drula R, Gulei D, Raduly L, et al. A Comprehensive Review on MAPK: A Promising Therapeutic Target in Cancer. Cancers (Basel). 2019 Oct 22;11(10). doi: 10.3390/cancers11101618
- Pfizer Inc. MEKTOVI® (bimetinib) [package insert]. US Food and Drug Administration website. https://bit.ly/3lHHkIY. Revised January 2019. Accessed February 16, 2023.
- Novartis AG. MEKINIST® (trametinib) [package insert]. US Food and Drug Administration website. https://bit.ly/3xrwtoX. Revised June 2022. Accessed February 16, 2023.
- AstraZeneca plc. KOSELUGO® (selumetinib) [package insert]. US Food and Drug Administration website. https://bit.ly/3I6b3mq. Revised 2021. Accessed February 16, 2023.
- Genentech, Inc. COTELLIC® (cobimetinib) [package insert]. US Food and Drug Administration website. https://bit.ly/3I9Uru9. Revised October 2022. Accessed February 16, 2023.
- Kuznetsova AV, Kurinov AM, Aleksandrova MA. Cell models to study regulation of cell transformation in pathologies of retinal pigment epithelium. J Ophthalmol. 2014;2014:801787. doi: 10.1155/2014/801787
- Tabernero J, Grothey A, van Cutsem E, Yaeger R, Wasan H, Yoshino T, et al. Encorafenib plus cetuximab as a new standard of care for previously treated BRAF V600E-mutant metastatic colorectal cancer: Updated survival results and subgroup analyses from the BEACON study. J Clin Oncol. 2021;39(4):273-284. doi: 10.1200/JCO.20.02088
- Kim R, McDonough S, El-Khoueiry A, Bekaii-Saab T, Stein S, Sahai V, et al. Randomised phase II trial (SWOG S1310) of single agent MEK inhibitor trametinib Versus 5-fluorouracil or capecitabine in refractory advanced biliary cancer. European journal of cancer (Oxford, England : 1990). 2020; 130:[219‐227 pp.]. doi: 10.1016/j.ejca.2020.01.026.
- Carvajal R, Piperno-Neumann S, Kapiteijn E, Chapman P, Frank S, Joshua A, et al. Selumetinib in Combination With Dacarbazine in Patients With Metastatic Uveal Melanoma: a Phase III, Multicenter, Randomized Trial (SUMIT). J Clin Oncol. 2018; 36(12):[1232‐1239 pp.]. doi: 10.1200/JCO.2017.74.1090.
- Dummer R, Ascierto PA, Gogas HJ, Arance A, Mandala M, Liszkay G, et al. Overall survival in patients with BRAF-mutant melanoma receiving encorafenib plus binimetinib versus vemurafenib or encorafenib (COLUMBUS): a multicentre, open-label, randomised, phase 3 trial. The Lancet Oncology. 2018;19(10):1315-1327. doi: 10.1016/S1470-2045(18)30497-2
- Van Cutsem E, Hidalgo M, Canon JL, Macarulla T, Bazin I, Poddubskaya E, et al. Phase I/II trial of pimasertib plus gemcitabine in patients with metastatic pancreatic cancer. Int J Cancer. 2018 Oct 15;143(8):2053-2064. doi: 10.1002/ijc.31603
- de la Cruz-Merino L, Di Guardo L, Grob JJ, Venosa A, Larkin J, McArthur GA, et al. Clinical features of serous retinopathy observed with cobimetinib in patients with BRAF-mutated melanoma treated in the randomized coBRIM study. J Transl Med. 2017 Jun 24;15(1):146. doi: 10.1186/s12967-017-1246-0
- Dréno B, Ribas A, Larkin J, Ascierto PA, Hauschild A, Thomas L, et al. Incidence, course, and management of toxicities associated with cobimetinib in combination with vemurafenib in the coBRIM study. Ann Oncol. 2017 May 1;28(5):1137-1144. doi: 10.1093/annonc/mdx040
- Carter C, Rajan A, Keen C, Szabo E, Khozin S, Thomas A, et al. Selumetinib with and without erlotinib in KRAS mutant and KRAS wild-type advanced nonsmall-cell lung cancer. Ann Oncol. 2016; 27(4):[693‐699 pp.]. doi: 10.1093/annonc/mdw008.
- Zaman K, Winterhalder R, Mamot C, Hasler-Strub U, Rochlitz C, Mueller A, et al. Fulvestrant with or without selumetinib, a MEK 1/2 inhibitor, in breast cancer progressing after aromatase inhibitor therapy: A multicentre randomised placebo-controlled double-blind phase II trial, SAKK 21/08. Eur J Cancer. 2015;51(10):1212-1220. doi: 10.1016/j.ejca.2015.03.016
- Robert C, Karaszewska B, Schachter J, Rutkowski P, Mackiewicz A, Stroiakovski D, et al. Improved overall survival in melanoma with combined dabrafenib and trametinib. N Engl J Med. 2015 Jan 1;372(1):30-39. doi: 10.1056/NEJMoa1412690
- Carvajal R, Sosman J, Quevedo J, Milhem M, Joshua A, Kudchadkar R, et al. Effect of selumetinib vs chemotherapy on progression-free survival in uveal melanoma: a randomized clinical trial. JAMA. 2014; 311(23):[2397‐2405 pp.]. doi: 10.1001/jama.2014.6096.
- Long GV, Stroyakovskiy D, Gogas H, Levchenko E, De Braud F, Larkin J, et al. Combined BRAF and MEK inhibition versus BRAF inhibition alone in melanoma. N Engl J Med. 2014;371(20):1877-1888. doi: 10.1056/NEJMoa1406037
- Gupta A, Love S, Schuh A, Shanyinde M, Larkin JM, Plummer R, et al. DOC-MEK: a double-blind randomized phase II trial of docetaxel with or without selumetinib in wild-type BRAF advanced melanoma. Ann Oncol. 2014 May;25(5):968-974. doi: 10.1093/annonc/mdu054
- Infante JR, Somer BG, Park JO, Li CP, Scheulen ME, Kasubhai SM, et al. A randomised, double-blind, placebo-controlled trial of trametinib, an oral MEK inhibitor, in combination with gemcitabine for patients with untreated metastatic adenocarcinoma of the pancreas. Eur J Cancer. 2014 Aug;50(12):2072-2081. doi: 10.1016/j.ejca.2014.04.024
- Robert C, Dummer R, Gutzmer R, Lorigan P, Kim KB, Nyakas M, et al. Selumetinib plus dacarbazine versus placebo plus dacarbazine as first-line treatment for BRAF-mutant metastatic melanoma: a phase 2 double-blind randomised study. Lancet Oncol. 2013 Jul;14(8):733-740. doi: 10.1016/S1470-2045(13)70237-7
- Flaherty KT, Robert C, Hersey P, Nathan P, Garbe C, Milhem M, et al. Improved survival with MEK inhibition in BRAF-mutated melanoma. N Engl J Med. 2012 Jul 12;367(2):107-114. doi: 10.1056/NEJMoa1203421
- Flaherty KT, Infante JR, Daud A, Gonzalez R, Kefford RF, Sosman J, et al. Combined BRAF and MEK inhibition in melanoma with BRAF V600 mutations. N Engl J Med. 2012 Nov 1;367(18):1694-1703. doi: 10.1056/NEJMoa1210093
- Alluri N, Jimeno A. Trametinib for the treatment of melanoma. Drugs of Today. 2013;49(8):491-498. doi: 10.1358/dot.2013.49.8.1990151
- Rinehart J, Adjei AA, Lorusso PM, Waterhouse D, Hecht JR, Natale RB, et al. Multicenter phase II study of the oral MEK inhibitor, CI-1040, in patients with advanced non-small-cell lung, breast, colon, and pancreatic cancer. J Clin Oncol. 2004 Nov 15;22(22):4456-4462. doi: 10.1200/JCO.2004.01.185
- LoRusso PM, Krishnamurthi SS, Rinehart JJ, Nabell LM, Malburg L, Chapman PB, et al. Phase I pharmacokinetic and pharmacodynamic study of the oral MAPK/ERK kinase inhibitor PD-0325901 in patients with advanced cancers. Clin Cancer Res. 2010;16(6):1924-1937. doi: 10.1158/1078-0432.CCR-09-1883
- Deming DA, Cavalcante LL, Lubner SJ, Mulkerin DL, Loconte NK, Eickhoff JC, et al. A phase i study of selumetinib (AZD6244/ARRY-142866), a MEK1/2 inhibitor, in combination with cetuximab in refractory solid tumors and KRAS mutant colorectal cancer. Invest New Drugs. 2016;34(2):168-175. doi: 10.1007/s10637-015-0314-7
- Long GV, Stroyakovskiy D, Gogas H, Levchenko E, de Braud F, Larkin J, et al. Dabrafenib and trametinib versus dabrafenib and placebo for Val600 BRAF-mutant melanoma: a multicentre, double-blind, phase 3 randomised controlled trial. Lancet. 2015 Aug 1;386(9992):444-451. doi: 10.1016/S0140-6736(15)60898-4
- Infante JR, Fecher LA, Falchook GS, Nallapareddy S, Gordon MS, Becerra C, et al. Safety, pharmacokinetic, pharmacodynamic, and efficacy data for the oral MEK inhibitor trametinib: a phase 1 dose-escalation trial. Lancet Oncol. 2012 Aug;13(8):773-781. doi: 10.1016/s1470-2045(12)70270-x
- Niro A, Strippoli S, Alessio G, Sborgia L, Recchimurzo N, Guida M. Ocular Toxicity in Metastatic Melanoma Patients Treated With Mitogen-Activated Protein Kinase Kinase Inhibitors: A Case Series. Am J Ophthalmol. 2015 Nov;160(5):959-967.e951. doi: 10.1016/j.ajo.2015.07.035
- Haura EB, Ricart AD, Larson TG, Stella PJ, Bazhenova L, Miller VA, et al. A phase II study of PD-0325901, an oral MEK inhibitor, in previously treated patients with advanced non-small cell lung cancer. Clin Cancer Res. 2010 Apr 15;16(8):2450-2457. doi: 10.1158/1078-0432.Ccr-09-1920
- Francis JH, Diamond EL, Chi P, Jaben K, Hyman DM, Abramson DH. MEK Inhibitor-Associated Central Retinal Vein Occlusion Associated with Hyperhomocysteinemia and MTHFR Variants. Ocul Oncol Pathol. 2020 May;6(3):159-163. doi: 10.1159/000501155
- Shields CL, Manalac J, Das C, Ferguson K, Shields JA. Choroidal melanoma: clinical features, classification, and top 10 pseudomelanomas. Curr Opin Ophthalmol. 2014 May;25(3):177-185. doi: 10.1097/ICU.0000000000000041
- Yip H, Chan E. Optical coherence tomography imaging in keratoconus. Clin Exp Optom. 2019 May;102(3):218-223. doi: 10.1111/cxo.12874
- Hayreh SS. Pathogenesis of optic disc edema in raised intracranial pressure. Prog Retin Eye Res. 2016 Jan;50:108-144. doi: 10.1016/j.preteyeres.2015.10.001
- Touhami S, Leclercq M, Stanescu-Segall D, Touitou V, Bodaghi B. Differential Diagnosis of Vitritis in Adult Patients. Ocul Immunol Inflamm. 2021 May 19;29(4):786-795. doi: 10.1080/09273948.2021.1898001
- Marcucci R, Sofi F, Grifoni E, Sodi A, Prisco D. Retinal vein occlusions: a review for the internist. Intern Emerg Med. 2011 Aug;6(4):307-314. doi: 10.1007/s11739-010-0478-2
- Scott IU, Campochiaro PA, Newman NJ, Biousse V. Retinal vascular occlusions. Lancet. 2020 Dec 12;396(10266):1927-1940. doi: 10.1016/S0140-6736(20)31559-2






 Presenting With Bone-Only Metastases")






