Practice-Changing and Reaffirming Data Set Up an Exciting Future in Melanoma
Positive data readouts from studies such as the phase 2/3 RELATIVITY-047 trial with relatlimab and nivolumab, and the phase 3 KEYNOTE-716 trial with pembrolizumab, cemented 2021 as a banner year for the treatment of patients with melanoma, across various stages and subtypes.


Meredith McKean, MD, MPH

Positive data readouts from studies such as the phase 2/3 RELATIVITY-047 trial (NCT03470922) with relatlimab and nivolumab (Opdivo), and the phase 3 KEYNOTE-716 trial (NCT03553836) with pembrolizumab (Keytruda), cemented 2021 as a banner year for the treatment of patients with melanoma, across various stages and subtypes, according to Meredith McKean, MD, MPH.
Specifically, data from the RELATIVITY-047 concerned patients with untreated metastatic or unresectable melanoma who received a fixed-dose combination of the LAG3-blocking antibody relatlimab plus nivolumab or nivolumab alone. The data were stratified by mutational profiles including LAG3 expression on immune cells, PD-L1 expression on tumor cells, and BRAF status (TABLE).1 The KEYNOTE-716 data highlighted the use of pembrolizumab as adjuvant treatment for patients with resected high-risk stage II melanoma vs placebo.
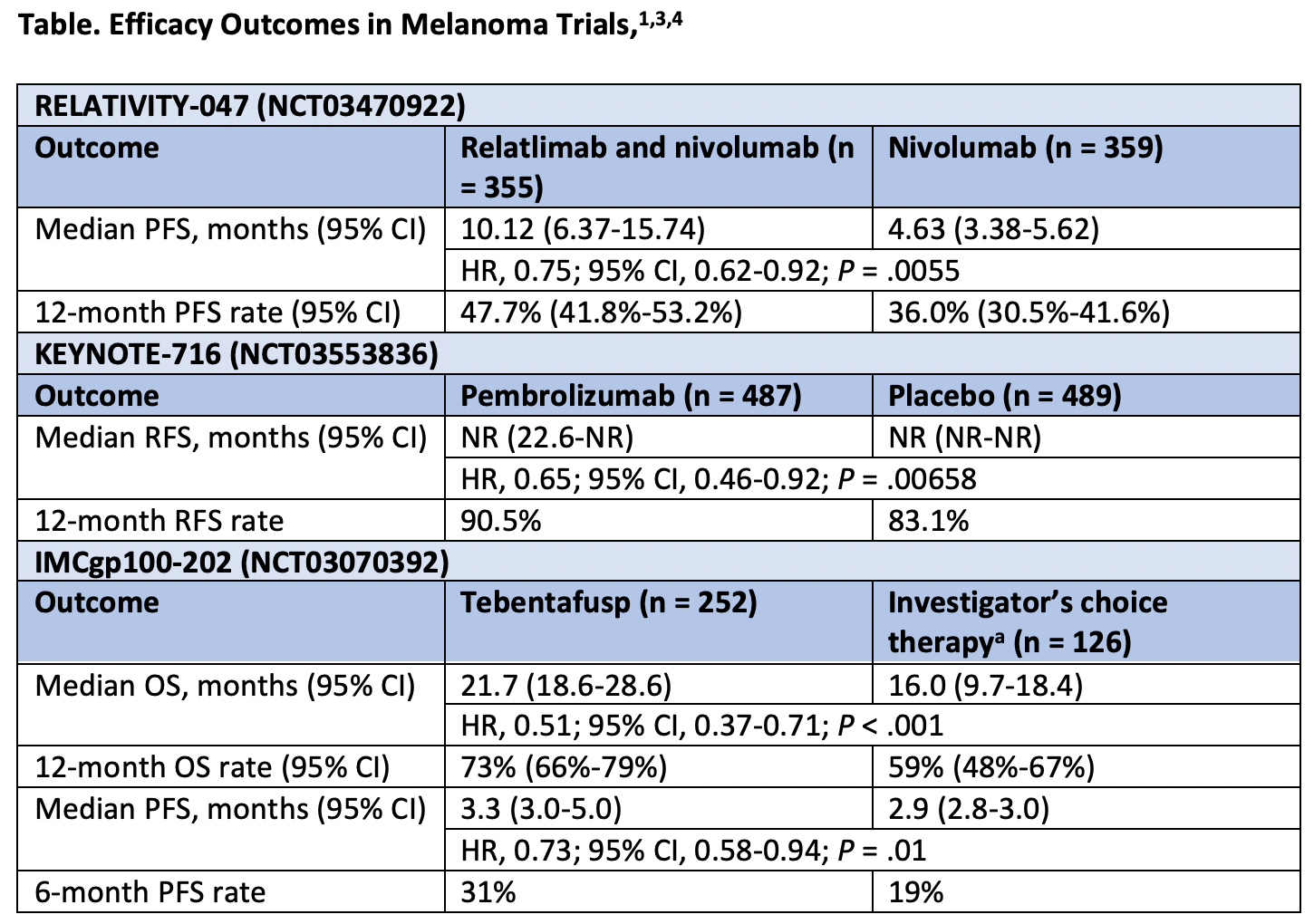
At the European Society for Medical Oncology Annual Congress 2021 investigators presented updated efficacy findings from RELATIVITY-047 which showed that patients who received a fixed-dose combination relatlimab and nivolumab (n = 355) had superior progression-free survival (PFS) and a tolerable safety profile compared with those who received nivolumab alone (n = 359). Specifically, the median PFS was 10.12 months (95% CI, 6.37-15.74) vs 4.63 months (95% CI, 3.38-5.62), respectively (HR, 0.75; 95% CI, 0.62-0.92; P = .0055).1 Based on these data, the FDA. granted a priority review to the biologics license application for the combination as treatment for adult and pediatric patients 12 years and older weighing at least 40 kg who have unresectable or metastatic melanoma.2
Recurrence-free survival (RFS) data from KEYNOTE-716 supported the use of adjuvant pembrolizumab for patients with earlier stage disease who have a high risk of recurrence similar to that among those with stage IIIA and IIIB melanoma. The median RFS was not reached (NR) in either arm of the trial: pembrolizumab (n = 487; 95% CI, 22.6-NR) vs placebo (n = 475; 95% CI, NR-NR). In the pembrolizumab arm 11.1% of patients experienced RFS events compared with 16.8% among those in the placebo arm (HR, 0.65; 95% CI, 0.46-0.92;P = .00658).3 The 12-month RFS rates were 90.5% vs 83.1%, respectively.
In an interview with OncLiveâ, McKean, the associate director of the Melanoma and Skin Cancer Research Program at Sarah Cannon Research Institute at Tennessee Oncology, discussed the most pivotal data for the treatment of patients with melanoma that read out in 2021 (TABLE1,3,4), and what is on the horizon for the space in 2022.


Table. Efficacy Outcomes in Melanoma Trials1,3,4
OncLive: In your opinion, what have been the most notable or practice changing studies in melanoma in 2021?
McKean: 2021 has been a big year for melanoma, and that has been exciting. We could see in the years leading up to 2021 that more progress was being made in some of the immunotherapy studies, so it has been exciting to see some breakthroughs.
The biggest headline [of 2021] is the RELATIVITY-047 trial. This [study examined] relatlimab, which is an anti-LAG3 monoclonal antibody, plus nivolumab, as a first-line therapy for patients with previously untreated metastatic melanoma. [The] combination [was examined] vs single-agent nivolumab. [The study has] been presented at 2 conferences at this point, [and results have demonstrated] a more than doubling of the PFS benefit vs single-agent nivolumab, which is exciting. The data [has shown that the combination has] been well tolerated, and this could be a great option for patients in the future.
There are still several questions remaining, and we are still waiting to see more data on response rates, and overall survival [OS]. Ipilimumab [Yervoy] plus nivolumab is still the bar for the frontline treatment of melanoma, so where this combination fits in the paradigm is still a big question.
Another study that was exciting to see was the KEYNOTE-716 trial. This was a phase 3 study of pembrolizumab [Keytruda] for patients with stage IIB and stage IIC melanoma. We have known that this is a patient population with a high risk of recurrence, so it was exciting to see the results demonstrating a 12-month RFS benefit in this group. This is still going to require a conversation with each patient, recognizing that we are still seeing the same toxicity that we have seen in other immunotherapy studies. Grade 3/4 toxicities [were reported in] approximately 16% [of patients on the study], so discussing with patients the RFS benefit vs some of the toxicities [will be important]. However, it is going to be great to have this option moving forward.
[Finally, the other] top study, in my opinion, was the phase 2 [IMCgp100-202] trial [(NCT03070392), which investigators examined] tebentafusp [IMCgp100] in patients with uveal melanoma. In the uveal melanoma space, it has been tough to try to find effective therapies, and this is the first treatment that has finally shown an OS benefit for this population. There are some caveats, however. The response rate was 9%, which may just indicate how difficult it is to assess response in these patients who tend to have a significant amount of disease in the liver. Also, this is still only going to be an option for approximately 50% of patients with metastatic uveal melanoma. Tebentafusp is a bispecific fusion protein targeting gp100 on tumor cells, and an anti-CD3 T cell–engaging domain, so it does require patients to have HLA-A*02:01–positive disease. For the patients that do not have that, this still will not be an option, but to finally see some progress in uveal melanoma has been exciting to see (Table1,3,4).
Please discuss long-term follow-up data from previous studies that we saw presented this year.
There was quite a bit of long-term [follow-up] data presented throughout the year. We saw the 6.5-year benefit of ipilimumab plus nivolumab [from the phase 3 CheckMate 067 trial (NCT01844505)]. It was exciting to see that at 6.5 years out, approximately 50% of patients are still alive. That was a huge landmark for patients with melanoma, their family members, and researchers to see how far we have come, but also to see how far we still have to go.
There were also several long-term follow-ups for some of the stage 3 adjuvant studies, such as the phase 3 KEYNOTE-054 trial [NCT023625940] with pembrolizumab, and the phase 3 CheckMate 915 trial [NCT03068455] with nivolumab. [These trials] affirmed that we continue to see a RFS benefit in the stage III population, which has been nice. Furthermore, we are continuing to see more data on how to manage stage IV, resected patients with brain metastases. We saw the phase 2 IMMUNED trial [NCT02523313] demonstrating the benefit [of treatment with] ipilimumab and nivolumab. There were a lot of studies this year that reaffirmed some of the practices that we had started implementing from that early data.
Is there any research that you are currently involved in and would like to highlight?
There is a lot of exciting research ongoing for cutaneous melanoma, as well as great interest in some of the more challenging subtypes. We are seeing excitement for some of the mRNA vaccines, some novel immunotherapy combinations, and [efforts] trying to target molecular drivers that previously had not been targets, such as patients with NRAS mutations, for example. [Additionally,] reaching out into these rarer subtypes, like uveal melanoma, after having some early success with tebentafusp, and seeing several other targeted therapy trials and specific treatment options just for those patients, has been really exciting to be a part of.
As we head into 2022, what is on the horizon for melanoma?
There are a couple of exciting areas. In the metastatic setting, we are waiting on additional results and follow-up from the phase 3 [PIVOT IO 001] study [NCT03635983] examining NKTR-214 [(bempegaldesleukin) plus nivolumab] in the frontline setting. That is going to be an exciting study to watch.
In a different space, the work that is being done in neoadjuvant melanoma has been exciting to see. That is a fascinating space, because we have seen in other tumor types that [neoadjuvant therapy is] beneficial for patients. The learning that is involved in being able to understand how these compounds work, which patients are benefiting, and the strides that are being made there, has been exciting to follow. We are learning so much about which combinations look to be beneficial, and that oftentimes, radiographic responses are underestimating pathologic responses. We are also learning a lot about tolerability and the immune response in that very early setting, so we are going to continue to see more and more in that space.
OS, overall survival; PFS, progression-free survival; RFS, recurrence-free survival. aInvestigator’s choice included single-agent pembrolizumab, ipilimumab, or dacarbazine.
References
- Hodi FS, Tawbi H, Lipson E, et al. Relatlimab (RELA) + nivolumab (NIVO) vs. NIVO in previously untreated metastatic or unresectable melanoma: additional efficacy in RELATIVITY-047. Ann Oncol. 2021;32(suppl 5):S867-S868. doi:10.1016/j.annonc.2021.08.1421
- US Food and Drug Administration accepts for priority review Bristol Myers Squibb’s application for LAG-3-blocking antibody relatlimab and nivolumab fixed-dose combination as treatment for patients with unresectable or metastatic melanoma. News release. Bristol Myers Squibb. September 20, 2021. Accessed November 20, 2021. bit.ly/3tVGyYG
- Luke JJ, Rutkowski P, Queirolo P, et al. Pembrolizumab versus placebo after complete resection of high-risk stage II melanoma: efficacy and safety results from the KEYNOTE-716 double-blind phase III trial. Ann Oncol. 2021;32(suppl 5):S1314-S1315. doi:10.1016/j.annonc.2021.08.2116
- Nathan P, Hassel JC, Rutkowski P, et al; IMCgp100-202 Investigators. Overall survival benefit with tebentafusp in metastatic uveal melanoma. N Engl J Med. 2021;385(13):1196-1206. doi:10.1056/NEJMoa2103485

 School of Medicine & Health Sciences")



















