

The Effect of Mindfulness on Outcomes in Psychiatric Patients
How can mindfulness-based intervention be used as an effective treatment option for psychiatric patients?


meditating-vector_biscotto87/Adobe Stock

What is Mindfulness?
The word, mindfulness, has its origins in the Sanskrit sati, which refers to awareness, attention, or alertness, and vipassanā, which means insight cultivated by meditation. An ancient Buddhist practice, mindfulness gained acceptance in traditional Western medicine and society in the 1970s through the work of Jon Kabat-Zinn.
Considered the “master of mindfulness,” Kabat-Zinn defines mindfulness as “an awareness that emerges through paying attention on purpose, in the present moment and non-judgmentally, to the unfolding of experience moment by moment.”1 This definition highlights the 3 tenets of mindfulness: 1) give undivided attention; 2) be aware of present thoughts and emotions; 3) accept them without judgment. Elements of mindfulness are incorporated commonly in practices such as yoga, meditation, relaxation, and breathing exercises,2 all of which are focused on grounding and directing and redirecting attention, with the goal of achieving harmony between the mind, the body, and the environment for improved health outcomes. Mindfulness can be practiced anytime, anywhere, and by anyone through full engagement in the here and now.
Measuring Mindfulness
Self-reported instruments/questionnaires are often used to assess mindfulness as: 1) a single-factor trait (eg, the Mindful Attention Awareness Scale) or state construct (eg, the Toronto Mindfulness Scale), or 2) a multi-construct concept with subscales capturing skills/tenets of mindfulness (eg, the Kentucky Inventory of Mindfulness Skills) or underlying coping processes (eg, the Applied Mindfulness Process Scale). Operationalization of mindfulness, especially when using multi-construct instruments, is important in that it allows exploration of underlying mechanisms of action, which helps inform the design of psychotherapeutic approaches and mindfulness-based interventions (eg, improve positive emotional regulation) to better increase effectiveness of treatment by focusing on components responsible for treatment effects.3
Clinical Value and Cognitive Aspects of Baseline Mindfulness
Understanding the benefits of mindfulness in psychiatric patient populations is important, as it offers clinicians a nonpharmacological therapeutic venue to address mental health issues deriving from living with chronic psychiatric, psychological, or neurological conditions, or from providing care to someone with these conditions such as Alzheimer disease and related dementias (ADRD), depression, or social anxiety. Determining patients’ baseline mindfulness facilitates identification of those most likely to benefit from mindfulness-based interventions to improve psychological outcomes, and it helps mental health providers better understand how patients may respond to treatment. In addition, baseline mindfulness may help providers better understand patterns of patients self-reporting their symptoms, or how they perform on cognitive and psychological testing during the initial office visit.4 In patients with ADRD, for example, higher baseline mindfulness predicts better cognitive performance and less severe cognitive impairment, likely via better positive emotional regulation, greater engagement in brain-protective behaviors such as physical activity and socialization, lower frailty, and cardiovascular risk, and greater resilience.4
Mindfulness has been consistently linked to psychosocial outcomes including higher life satisfaction, lower depression, dissociation, social anxiety, and rumination, and better cognitive processes such as lower frequency of negative automatic thoughts, with important implications for psychological health.5 Finally, regular engagement in mindfulness practice is positively linked to psychological well-being, cognitive flexibility, and attentional functioning and negatively associated with psychological symptoms including rumination, thought suppression, and difficulties with emotion regulation.6 Thus, understanding and applying aspects of mindfulness during patient evaluations provides another useful tool for practicing psychiatrists and other mental health providers.
Mindfulness-Based Therapies
The observed link with psychological and other health outcomes led to the development of several mindfulness-based therapies to address these health concerns. Mindfulness-based stress reduction (MBSR), the first therapeutic modality championed by Kabat-Zinn in the 80s and 90s for treatment of patients with chronic pain, is an 8- to 10-week group program engaging participants in mindfulness meditation training and practice with the goal of becoming less reactive, more acceptant of their own experiences, and more able to disengage from maladaptive behaviors and thoughts and to reduce negative experiences through cognitive reappraisal.1
Mindfulness-based cognitive therapy (MBCT) was developed for the treatment of remitted depression and combines mindfulness training with elements of cognitive therapy with the goal of changing awareness of and relationship to thoughts and emotions7 and “breaking” the association between negative automatic thinking and dysphoria.5 Dialectical behavior therapy (DBT), first developed as a treatment for chronic suicidality, integrates elements of traditional cognitive-based therapy (CBT), Zen practice, and mindfulness skill training to improve emotional regulation and increase patient self-acceptance through a combination of behavior change (CBT), acceptance-oriented (Zen) strategies, and coping skill training (mindfulness).8
Benefits of Mindfulness-Based Interventions
The robust positive relationships observed in observational studies between mindfulness and various psychological and cognitive outcomes are supported by reports from mindfulness-based interventions (Table). There is consistent evidence for a positive effect of MBSR on mood (reduced anxiety and depression), stress (reduced distress), cognition (improved performance), and overall wellbeing (improved satisfaction with life and quality of life) in nonclinical (eg, students, community-dwelling adults, health care professionals) and clinical (eg, patients with fibromyalgia, cancer, social anxiety, bipolar disorder, and neurological conditions) populations.9 These findings are further supported by observed brain changes in areas associated with emotional regulation in participants receiving MBSR compared to controls.10


Table. Psychiatric Conditions and Outcomes Impacted by Mindfulness-Based Interventions
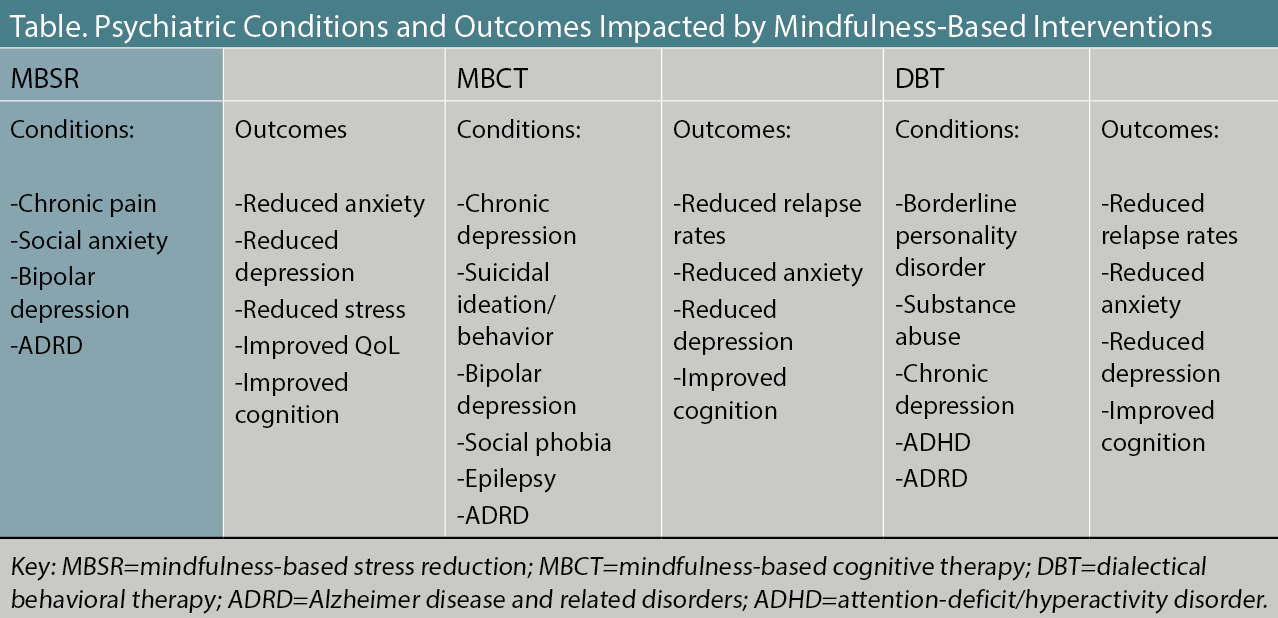
Initial studies of MBCT in patients with major depression found compelling evidence for reductions in relapse rates in those receiving MBCT interventions,7 reductions that may be similar to what is observed in patients on pharmacotherapy, with effects significantly improved when the 2 are combined.11 Despite this evidence, pharmacotherapy remains the main treatment option for many patients with mental disorders, although ~75% of patients with mental disorders prefer psychotherapy.12
More recently, clinical trials on MBCT have expanded their investigation into other psychosocial outcomes, reporting benefits on anxiety, depressive mood, quality of life, symptoms of social phobia, cognition, metacognitive awareness, and thought suppression in patients with recurrent depression,13 as well as other psychiatric conditions including suicidal ideation or behavior, bipolar depression, social phobia, and epilepsy.5 Imaging studies confirmed increased activation following MBCT in brain areas such as the medial prefrontal cortex, which is involved in emotional processing and self-referential mental activities.14
Similarly, DBT therapy has been found to be successful in reducing suicidal ideation and behavior and self-harm behavior including drug use, self-mutilation, and binge-eating in patients with borderline personality behavior,8 comorbid substance dependence, bulimia, depression,5 and more recently in patients with attention-deficit/hyperactivity disorder.15 Benefits on other psychological outcomes include reduced depression, anxiety, hopelessness, dissociation, anger, and improved global social adjustment and functioning, and adaptive coping.5,8 Providing further evidence for an impact of DBT on psychological outcomes, pre-post intervention changes in the brain including reduction in amygdala activation16 and alteration of grey matter in regions of the brain that are implicated in emotion regulation and higher-order functions following DBT were reported in patients with borderline personality disorder.17
Finally, mindfulness-based interventions have been found to improve cognitive and psychosocial outcomes in patients with ADRD and their caregivers, who both suffer from increased stress, depression, anxiety, and burden either from having the disease or from providing care for someone with the disease, with further negative impact on health and wellbeing. The evidence is consistent in showing that older adults with ADRD participating in MBI have improved cognitive function18 and psychosocial functioning including depressive and anxious symptomatology and perceived stress.2 Mindfulness-based interventions in individuals who provide round-the-clock care to patients with ADRD were shown to produce improvements in stress, burden, mood, and quality of life.2,19 When done simultaneously in patients and caregivers, mindfulness-based interventions are successful at improving mood and quality of life in both, supporting a crossover of effects from caregivers to patients.20
Case Vignette
George is a 70-year-old retired educator who sought therapy for depression and anxiety related to a 2018 diagnosis of ADRD. The diagnostic interview indicated that he suffers from depression and anxiety due to another medical condition according to the DSM-V. During the initial session, George complained about increased apathy, a feeling of despair, and a struggle to find meaning in the time he has left. He reported a constant worry surrounding a gradual loss of cognitive function impeding his ability to drive, sleep, and participate in activities he used to enjoy including long-distance bike riding.
Goals of treatment included use of mindfulness-based modalities (MBSR, DBT, and MBCT) to:
-Increase insight of depressive and anxious feelings.
-Teach George to identify automatic negative thoughts (ANTS) and learn to reframe them.
-Accept the disease.
-Improve problem solving concerning return to physical activities he enjoys.
Mindfulness techniques used:
-Meditation: George participated in short meditations specifically targeting awareness of feelings and anxiety reduction, gradually increasing insight, and understanding of his feelings and emotions.
-Reframing ANTS: Recording situations preceding ANTS eventually taught George to fact-check the dysfunctional thoughts and challenge their validity.
-Journaling: George journaled his struggle with acceptance of the disease, including moments of gratefulness he encountered throughout his week.
-Setting intention: George learned to set an intention every morning, checking in with himself throughout the day to course correct so he can stay on target.
Therapeutic achievements:
George was open-minded and cooperative with the treatment, and the therapeutic results were remarkable. After a month of weekly sessions, George resumed his long-distance bike rides and other physical actives he enjoys. At the 3-month mark, he accepted his inability to drive and surrendered his driver’s license to his wife. After 10 months of mindfulness-based therapy, he sleeps well throughout the night, looks forward to meaningful interactions with his family and friends, and reports having “APTS: automatic positive thoughts” (his own term), as opposed to ANTS. He set alarms on his phone to “jump for joy” in the morning and to “be grateful” in the afternoon.
Conclusion
There is compelling evidence to support mindfulness-based intervention as an effective treatment option in psychiatric patients either on its own or in combination with psychiatric medications. Psychotherapeutic approaches are found to be efficacious in a variety of psychiatric disorders and can address a multitude of psychosocial and cognitive challenges that are common in this patient population. Treatment decisions should take into consideration the patient’s baseline mindfulness, which can be easily assessed in the clinical setting, to determine which patients are likely to benefit from mindfulness and other therapies or to inform the clinician on patterns of response to treatment. Patients suffering from chronic conditions and those providing care to them respond well to psychotherapy and are reported to prefer it to pharmacotherapy.
Integration of nonpharmacological mindfulness-based treatment options that are backed by robust evidence of effectiveness in reducing anxiety, depression, stress, and burden, and in improving quality of life offers patients effective therapies that are generally considered safer and have fewer side effects. In addition, in the subset of psychiatric patients with cognitive impairment, mindfulness-based therapies may help maintain or even improve cognitive function, therefore addressing a significant public health concern in the geriatric population.
Dr Tolea is a research assistant professor and associate director of research at the Comprehensive Center for Brain Health, Cognitive Disorders Division, University of Miami Miller School of Medicine. Ms Cohen is a social worker and community outreach coordinator in the Comprehensive Center for Brain Health, University of Miami Miller School of Medicine. Dr Galvin is a professor of neurology at the University of Miami Miller School of Medicine and founding director of the Comprehensive Center for Brain Health.
ACKNOWLEDGEMENTS AND FUNDING SOURCES
This study was supported by grants to JEG from the National Institute on Aging (R01 AG071514, R01 AG069765, R01 AG057681, and R01 NS101483), the Harry T. Mangurian Foundation, and the Leo and Anne Albert Charitable Trust. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
References
1. Kabat-Zinn J. An outpatient program in behavioral medicine for chronic pain patients based on the practice of mindfulness meditation: theoretical considerations and preliminary results. Gen Hosp Psychiatry. 1982;4(1):33-47.
2. Larouche E, Hudon C, Goulet S. Potential benefits of mindfulness-based interventions in mild cognitive impairment and Alzheimer's disease: an interdisciplinary perspective. Behav Brain Res. 2015;276:199-212.
3. Baer RA. Measuring mindfulness. Contemporary Buddhism. 2011;12(1):241-261.
4. Innis AD, Tolea MI, Galvin JE. The effect of baseline patient and caregiver mindfulness on dementia outcomes. J Alzheimers Dis. 2021;79(3):1345-1367.
5. Keng SL, Smoski MJ, Robins CJ. Effects of mindfulness on psychological health: a review of empirical studies. Clin Psychol Rev. 2011;31(6):1041-1056.
6. Lykins E, Baer RA. Psychological functioning in a sample of long-term practitioners of mindfulness meditation. J Cogn Psychother. 2009;23(3):226-241.
7. Teasdale JD, Segal ZV, Williams JM, et al. Prevention of relapse/recurrence in major depression by mindfulness-based cognitive therapy. J Consult Clin Psychol. 2000;68(4):615-623.
8. Linehan MM, Korslund KE, Harned MS, et al. Dialectical behavior therapy for high suicide risk in individuals with borderline personality disorder: a randomized clinical trial and component analysis [published correction appears in JAMA Psychiatry. 2015;72(9):951]. JAMA Psychiatry. 2015;72(5):475-482.
9. Koszycki D, Benger M, Shlik J, Bradwejn J. Randomized trial of a meditation-based stress reduction program and cognitive behavior therapy in generalized social anxiety disorder. Behav Res Ther. 2007;45(10):2518-2526.
10. Davidson RJ, Kabat-Zinn J, Schumacher J, et al. Alterations in brain and immune function produced by mindfulness meditation. Psychosom Med. 2003;65(4):564-570.
11. Cuijpers P. Combined pharmacotherapy and psychotherapy in the treatment of mild to moderate major depression? JAMA Psychiatry. 2014;71(7):747-748.
12. McHugh RK, Whitton SW, Peckham AD, et al. Patient preference for psychological vs pharmacologic treatment of psychiatric disorders: a meta-analytic review. J Clin Psychiatry. 2013;74(6):595-602.
13. Orgeta V, Qazi A, Spector A, Orrell M. Psychological treatments for depression and anxiety in dementia and mild cognitive impairment: systematic review and meta-analysis. Br J Psychiatry. 2015;207(4):293-298.
14. Ives-Deliperi VL, Howells F, Stein DJ, et al. The effects of mindfulness-based cognitive therapy in patients with bipolar disorder: a controlled functional MRI investigation. J Affect Disord. 2013;150(3):1152-1157.
15. Fleming AP, McMahon RJ, Moran LR, et al. Pilot randomized controlled trial of dialectical behavior therapy group skills training for ADHD among college students. J Atten Disord. 2015;19(3):260-271.
16. Goodman M, Carpenter D, Tang CY, et al. Dialectical behavior therapy alters emotion regulation and amygdala activity in patients with borderline personality disorder. J Psychiatr Res. 2014;57:108-116.
17. Mancke F, Schmitt R, Winter D, et al. Assessing the marks of change: how psychotherapy alters the brain structure in women with borderline personality disorder. J Psychiatry Neurosci. 2018;43(3):171-181.
18. Quintana-Hernández DJ, Miró-Barrachina MT, Ibáñez-Fernández IJ, et al. Mindfulness in the maintenance of cognitive capacities in Alzheimer’s disease: a randomized clinical trial. J Alzheimers Dis. 2016;50(1):217-232.
19. Shim M, Tilley JL, Im S, et al. A systematic review of mindfulness-based interventions for patients with mild cognitive impairment or dementia and caregivers [published online ahead of print, 2020 Sep 16]. J Geriatr Psychiatry Neurol. 2020;891988720957104.
20. Paller KA, Creery JD, Florczak SM, et al. Benefits of mindfulness training for patients with progressive cognitive decline and their caregivers. Am J Alzheimers Dis Other Demen. 2015;30(3):257-267.















