


I had a milestone birthday recently.
A birthday which I refused to celebrate, threatened my husband and friends not to dare surprise me with any activities and had planned to spend alone on the couch with a Law and Order binge fest.
My 7-year-old Emmy, sensing my sadness, had better plans. She started my day with breakfast in bed, strong coffee and proclaimed we could spend time together with “cuddles and cries.”
With a little perspective from my youngest that my mood was being impacted, step one is recognition followed by a plan of action.
In a similar manner, we all know that mood disorders are common in nursing homes and are often underdiagnosed and undertreated.
Furthermore, appreciation of this fact and appropriate completion of MDS Section D: Mood is an essential step in promoting the interdisciplinary teams’ ability to address individual patient needs.
Finally, we know that the depression end split has a direct impact on case mix HIPPS under the Patient Driven Payment Model (PDPM).
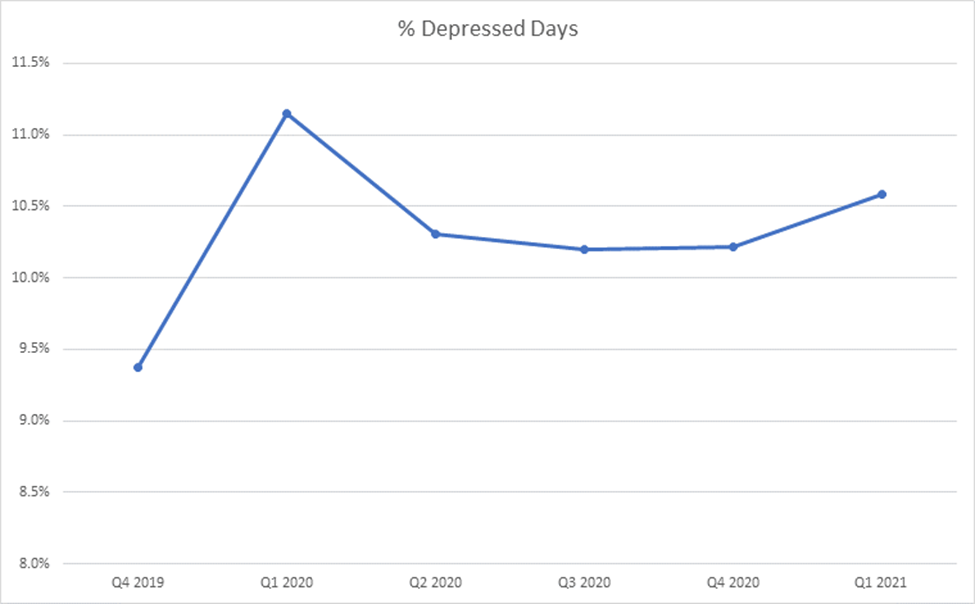
Curious as to how the nation has measured depression over the course of the pandemic and onset of PDPM? Below is a representation of current data trends per CMS Research Data Assistance Center (ResDAC)
Section D, the portion of the MDS which is used to assess mood, has a clear intent.
The items in this section address mood distress, a serious condition that is underdiagnosed and undertreated in the nursing home and also associated with significant morbidity.
Research evidence is presented in the Resident Assessment Instrument (RAI) Manual showing that depression can be associated with: psychological and physical distress (e.g., poor adjustment to the nursing home, loss of independence, chronic illness, increased sensitivity to pain), decreased participation in therapy and activities (e.g., caused by isolation), decreased functional status (e.g., resistance to daily care, decreased desire to participate in activities of daily living or ADLs), and poorer outcomes (e.g., decreased appetite, decreased cognitive status).
Based on these facts, it is evident that appreciation and review of Section D should be openly discussed across the rehab team, including therapy and nursing.
The 9-ITEM PATIENT HEALTH QUESTIONNAIRE (PHQ-9©) portion of Section D is a validated interview that screens for symptoms of depression. It provides a standardized severity score and a rating for evidence of a depressive disorder.
The questions here are not for the faint of heart: “Over the last two weeks, have you been bothered by any of of the following problems: little interest or pleasure in doing things, feeling down, depressed, or hopeless, trouble falling or staying asleep, or sleeping too much, feeling tired or having little energy…” and the list goes on.
While completion of portions of Section D, including the PHQ-9©, may be challenging and even emotionally difficult from an interviewer perspective, providers should not find them depressing. They are intended to act as a source for identifying interventions and causes to best support those we serve in our skilled nursing facilities.
Additionally, it is important to note that coding the presence of indicators in Section D does not automatically mean that the resident has a diagnosis of depression or other mood disorder. Assessors do not make or assign a diagnosis in Section D; they simply record the presence or absence of specific clinical mood indicators.
They should be viewed as a road map, a step in the right direction that allows us as caregivers to better understand and care for our patients daily.
It is particularly important to identify signs and symptoms of mood distress among nursing home residents because these signs and symptoms can be treatable. Facility staff should recognize these indicators and consider them when developing the resident’s individualized care plan.
Once areas are identified and a care plan is established, we can move forward addressing the residents’ needs; identify causes and contributing factors for symptoms; identify interventions (treatment, personal support, or environmental modifications) that could address symptoms; and ensure individual resident safety.
In closing, when you look at Section D as a whole, it’s not so depressing after all.
It is simply another source to better understand others, serve our patient population and meet them where they are, cuddles, cries, coffee and all.
Renee Kinder, MS, CCC-SLP, RAC-CT, is Executive Vice President of Clinical Services for Broad River Rehab and a 2019 APEX Award of Excellence winner in the Writing–Regular Departments & Columns category. Additionally, she serves as Gerontology Professional Development Manager for the American Speech Language Hearing Association’s (ASHA) gerontology special interest group, is a member of the University of Kentucky College of Medicine community faculty and is an advisor to the American Medical Association’s Relative Value Update Committee (RUC) Health Care Professionals Advisory Committee (HCPAC).
The opinions expressed in McKnight’s Long-Term Care News guest submissions are the author’s and are not necessarily those of McKnight’s Long-Term Care News or its editors.





